

Case Report
Congenital Ureterovaginal Fistula Secondary to Ectopic Ureter – A Case Report
Daniyan ABC1, Obi AO1,2, Gokir N3, Nwoba V1, Ogbule I1, Daniyan OW2, Yakubu EN1, Obuna JA1
1National Obstetric Fistula Centre, Abakaliki, Nigeria
2Alex Ekwueme Federal University Teaching Hospital, Abakaliki, Nigeria
3Federal Medical Centre, Yola, Nigeria
ABSTRACT
INTRODUCTION
Urinary incontinence has a negative impact on a woman’s quality of life due to its enormous medical, economic, social and psychosexual consequences.1 Female genital fistula is an important cause of urinary incontinence in Nigeria and other low- and middle-income countries.2,3,4 While obstetric causes are responsible for the vast majority of genital fistulas among women in our environment,5,6,7 there are other causes which can constitute similar degree of nuisance in affected women. These are gynaecological procedures, direct trauma, pelvic malignancies, pelvic irradiation, chronic granulomatous infections, rape, neurofibromatosis and rarely congenital malformations.8,9,10 One of such congenital malformations is an ectopic ureter.11,12
An ectopic ureter is any ureter, single or duplex, that opens into places other than the bladder trigone.13 It is a rare congenital anomaly that is seen in about 1 in 1,900 people and is 10 times commoner in girls.14 It is familial with an offspring of an affected parent having a 50% chance of developing it. It is commoner on the left and can occur with a single kidney or a duplex kidney. About 80% are associated with duplex kidneys14 or a duplex collecting system,12 while about 20% are associated with a single collecting system.12 In females, the most common sites of insertion are the bladder neck, upper urethra, vestibule between the urethra and introitus, vagina, cervix and uterus; while in males the common sites are lower urinary bladder, posterior urethra, seminal vesicle, ductus deferens, ejaculatory duct and rectum.14,15 It presents with urinary incontinence due to delivery of urine to an abnormal location, recurrent urinary tract infections and abdominal swelling.16 It may however be asymptomatic.17 Even though it is present at birth, it is often not diagnosed until after several years. Diagnosis entails use of imaging techniques.17,18 Cystoscopy and renal flow scan may also be done. Treatment is surgical and it is aimed not only at treating the urinary incontinence, but also to prevent renal damage from obstructive uropathy and recurrent urinary tract infection. Postoperatively, the prognosis is good.
We present a case of ectopic ureter causing urinary incontinence since childhood but was diagnosed in adulthood and corrected surgically with good outcomes.
CASE PRESENTATION
A 20-year-old single Para 0+0 lady was referred with complaints of involuntary leakage of urine from the vaginal from birth. Her mother became worried when she could not achieve continence at 7 years of age. She experienced normal bladder filling and emptying, in addition to nocturnal and daytime urinary incontinence for which she was using diapers. There was no history of surgery, childbirth, termination of pregnancy, sexual abuse or trauma. There was no leakage of urine while sneezing. There was no leakage of faeces. She was taken to various hospitals to no avail, hence the referral. She attained menarche at 12 years. She was not a known hypertensive or diabetic. There was no known family history of congenital malformation.
On examination, her general condition was good and vital signs were normal. Her chest and abdominal findings were also normal. Her vulva and vagina were wet. There was no vaginal wall defect. Methylene blue dye test was negative. Cough impulse was negative. A tiny opening was seen on the left lateral aspect of the anterior vaginal wall spilling urine at regular intervals (Figure 1). A diagnosis of ureterovaginal fistula was made. She was counseled on the findings and diagnosis. Her haemoglobin, fasting blood sugar, serum electrolytes, urea and creatinine were all within normal limits. HIV, Hepatitis B and C screening were all negative. Urinalysis was essentially normal. Urine culture was negative. Chest radiograph showed normal findings.
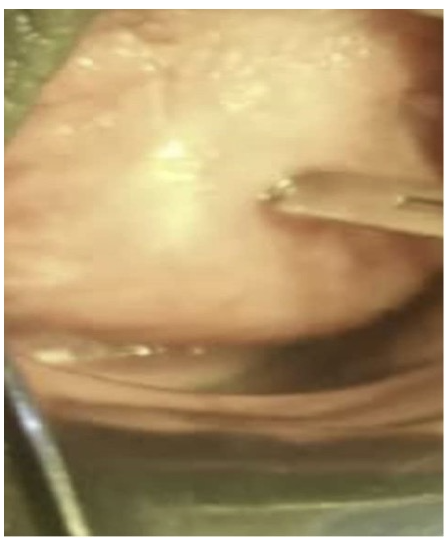
Figure 1 Opening of ectopic ureter on the anterior vaginal wall seen on speculum examination
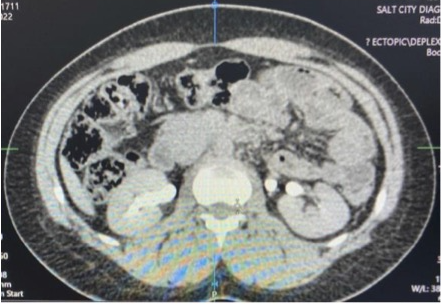
Figure 2 CT Urogram showing two ureters on the left and one on the right
Cystoscopy showed a well distended bladder with healthy bladder mucosa. Both ureteric openings were seen spilling urine. Computerized tomography urogram showed a normal-sized left kidney with complete duplex collecting system and duplex ureters. The upper moiety ureter inserted ectopically into the left lateral wall of the vagina. The ipsilateral lower moiety ureter inserted orthotopically. There was no filling defect or area of extrinsic constriction. The right kidney, collecting system, ureter and bladder were normal (Figures 2 and 3). A radiological assessment of left complete duplex collecting system with upper moiety ureter inserting into the vagina was made.

Figure 3 CT Urogram showing duplex collecting system on the left and extravesical insertion of the ectopic ureter
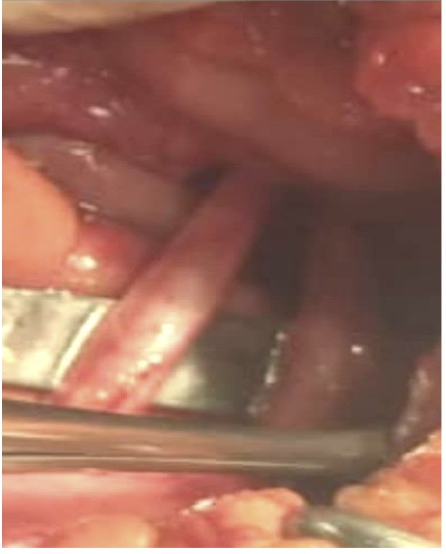
Figure 4 Two left ureters identified intraoperatively
A diagnosis of congenital ureterovaginal fistula secondary to an ectopic ureter was made. The patient was managed by urogynaecologists and urologists. The diagnosis was explained to her. She gave consent for ureteroneocystostomy under combined spinal epidural anaesthesia. She had exploratory laparotomy through a lower abdominal midline incision. She was found to have two left ureters (Figure 4), a smaller one that inserted normally into the bladder and a larger one that inserted through the Pouch of Douglas into the vagina. The orthotopic ureter was identified by passing a guide wire into the left ureteric orifice through the bladder incision. The ectopic ureter was freed, clamped and transected above its insertion into the upper vagina. A left ureteroneocystostomy was done by tunneling the ectopic ureter into the posterior bladder wall above the trigone. An improvised feeding tube stent was inserted into the new ureteric opening. The stent was anchored to the urethral catheter. The bladder was closed in two layers. Anterior abdominal wall was closed in layers. The catheter ureteric stent complex was removed after 7 days. A fresh catheter was passed which was removed after another 7 days. Postoperative dye test was negative, cough impulse was negative, patient was continent and was discharged home. She was seen three months later and she is continent.
DISCUSSION
Ectopic ureter is a rare congenital abnormality of the genitourinary tract, occurring in 1 in 1,900 people.14 It occurs when a ureter inserts outside the internal ureteral orifice at the trigine of the bladder.13 It results when the origin of the ureteric bud from the mesonephric (Wolfian) duct is abnormally high and separation of the bud from from the duct is delayed or fails to take place.14,17 It is usually associated in 80% of cases with a duplex collecting system.12 This was the case with the patient presented.
Ectopic ureter may result in urinary incontinence in a woman if the ureter inserts into the vagina as in the case reported. Urogynaecologists need to be familiar with this condition because it is 10 times commoner in females.14 Although it is present at birth, it is not usually diagnosed until later in life. It should therefore be considered in the differential diagnosis of urinary incontinence especially in a patient with normal bladder filling and emptying.
Nocturnal and daytime incontinence is usually a problem in the older child because the ureter continues to spill urine through the vaginal opening. In the patient presented, the mother became concerned when she could not achieve continence at 7 years of age. She had been taken to several hospitals before she was eventually referred for definitive treatment at 20 years of age. Early detection and treatment is important to restore continence and improve the patient’s quality of life as well as to prevent complications such as ureterocoele, recurrent urinary tract infection, hydronephrosis and obstructive uropathy. In this patient, the ectopic ureter was slightly larger than the normal one suggesting some obstruction at the vaginal opening.
Paradoxical urination is a feature of ureterovaginal fistula from an ectopic ureter. This occurs when a patient experiences normal voiding and also leaks urine uncontrollably. The patient experienced normal bladder filling and emptying in addition to the involuntary leakage of urine. Methylene blue dye test is usually employed in the diagnosis of genital fistulas. In this case, the test was negative. A negative dye test with a vagina that is wet with urine is strongly suggestive of ureterovaginal fistula. In our patient, a tiny opening was seen on the left lateral aspect of the anterior vaginal wall spilling urine at regular intervals. That was the opening of the ectopic ureter. Other sites of ectopic ureteric opening include the bladder neck, upper urethra, vestibule between the urethra and introitus, cervix and uterus.15
In some instances, it may be difficult or impossible to locate the opening of the ectopic ureter. Diagnosis may therefore require radiological imaging techniques such as computerized tomography urography, MRI urography or urethrocystography.11 In this patient, an ectopic ureteral opening was seen clinically on speculum examination. Further evaluation was however done using computerized tomography urography to confirm the diagnosis and further characterize the ureter. She also had cystoscopy which revealed two normal and functional ureteric openings in the bladder.
Management of ureterovaginal fistula from an ectopic ureter should be by a multidisciplinary team comprising urogynaecologists, urologists and radiologists as seen in this patient. The treatment is ureteroneocystostomy. This involves reimplanting the ureter into the bladder using standard techniques. She was discharged continent after 14 days.
In conclusion, congenital ectopic ureter, although rare, may cause involuntary leakage of urine in a woman if it inserts into the vagina. This has a profound negative impact on a patient’s quality of life. It should therefore be considered in the differential diagnosis of urinary incontinence. Since it is commoner in females, urogynaecologists should be familiar with its presentation and management. Radiological imaging is very important in the evaluation and best outcomes are achieved using a multidisciplinary approach.
REFERENCES
- Hu JS, Pierre EF. Urinary incontinence in women: evaluation and management. Am Fam Physician 2019; 100: 339-48.
- Daniyan B. Obstetric fistula – an unceasing scourge in the developing world. J Neonatal Biol 2017; 6: 244. doi: 10.4172/2167-0897.1000244.
- Stamatakos M, Sargedi C, Stasinou T, Kontzoglou. Vesocovaginal fistula: diagnosis and management. Indian J Surg 2014; 76: 131-6.
- Swain D, Parida SP, Jena SK, Das H. Obstetric fistula: a challenge to public health. Indian J Public Health 2019; 63: 73-8.
- Sunday-Adeoye I, Okonta P, Ogbonnaya L. Prevalence, profile and obstetric experience of fistula patients in Abakaliki, Southeast Nigeria. Urogynecologica 2011; 25: 20-4.
- Bello OO, Morhason-Bello IO, Ojengbede OA. Nigeria, a high burden state of obstetric fistula: a contextual analysis of key drivers. PAMJ 2020, 36.
- Daru PH, Karshima JA, Mikah S, Nyango D. The burden of vesico-vaginal fistula in North Central Nigeria. J West Afr Coll Surg 2011; 1: 50-62.
- El-Azab AS, Abolella HA, Farouk M. Update on vesicovaginal fistula: a systematic review. Arab J Urol 2019; 17: 61-8.
- Ekwedigwe K, Sunday-Adeoye I, Isikhuemen E, Daniyan B, Yakubu E. Spontaneous vesicovaginal fistula in neurofibromatosis: a case report. Gynecol Obstet (Sunnyvale) 2017; 7:421.
- Kochhar G, Ashwin SP, Reddy D, Gopalakrishnan G. Congenital vesicovaginal fistula – a rare cause of urinary incontinence in adulthood. Euro J Obst Gynecol 2021; 261: 252-3.
- Kuliniec I, Mitura P, Plaza P, Widz D, Sudol D, Godzisz M, Kolodynska A, Monist M, Wisz A, Bar K. Urinary incontinence in adulthood in a case of ectopic ureter – description of two clinical cases with review of literature. Int J Environ Res Public Health 2021; 18: 7084 doi: 10.3390/ijerph18137084
- Duicu C, Kiss E, Simu L, Aldea C. A rare case of double-system with ectopic ureteral openings into vagina. Front Pediatr 2018; 6: 176. doi: 10.3389/fped.2018.00176
- Jain P, Sarkar D, Maiti K, Gupta S, Pal DK. Rare case of ectopic ureter: analysis from a single centre with review of the literature. Turk J Urol 2019; 45: S92-S97.
- Abdrabou A, Foster T, El-Feky M, et al. Ectopic ureter. Reference article, Radiopaedia.org 2013 https://doi.org/10.53347/rID-24367 [Accessed on 20.12.2022 ]
- Balawender K, Wawrzyniak A, Pliszka A, Jozefiak A, Siwak S, Sokol D, Clarke E, Olszewska A, Mazur M, Mazurek A, Barszcz K, Zytkowski A. Ectopic ureter: a concise narrative review with anatomical and clinical commentaries. Translational Research in Anatomy 2022; 29: 100220. doi: 10.1016/j.tria.2022.100220
- Wang Q, Wu Z, Zhzng F, Akbar R, Lou Y, Zhou J, Ruan F. Gynecological diagnosis and treatment of ectopic ureter insertion into vagina. Analysis of five cases and a literature review. J Clin Med 2022; 11: 6267. doi: 10.3390/jcm11216267
- Baskin LS. Ectopic ureter. Up to date (2016). Available at: http://www.uptodate.com/contents/ectopic-ureter [Assessed on 20.12.2022]
- Sunday-Adeoye I, Ekwedigwe KC, Isikhuemen ME, Eliboh MO, Yakubu EN, Daniyan B. Intravenous urography findings in women with ureteric fistula. Pan Afr Med J 2018; 30: 203. doi: 10.11604/pamj.2018.30.203.1534