Corresponding author:
Saanu Olugbenga Oluseun
Department of Obstetrics and Gynaecology,
University College Hospital, Ibadan, Nigeria
saanuolu@yahoo.com
08033372153
INTRODUCTION
Contraception is the deliberate prevention of pregnancy despite unprotected sexual intercourse through the use of various devices, sexual practices, chemicals, drugs, or surgical procedures 1. It is described as effective if it allows a physical relationship without fear of unwanted pregnancy and ensures the freedom to have children when desired 1,2.
Contraceptive use confers many advantages, including adequate spacing of pregnancies and prevention of pregnancies in women at risk of adverse pregnancy outcomes 1,3. As important and useful as contraceptives are, there is still an unmet need for contraception globally. It was reported in 2014 that more than a 225million women in developing countries were unable to access and use family planning or contraception 3,4. The world health organization (WHO, 2020) identified gender-based barriers as one of the reasons for the unmet need for contraception, other reasons included: limited access to contraception, limited choice of methods, fear or experience of side effects, cultural or religious opposition, and poor quality of available services 5-8. Aliyu found out in Zaria, Northern Nigeria that although 97.7% of the interviewed 309 married women knew about contraception, the contraceptive prevalence rate was just 15.2% 9.
The gender-based barrier to contraceptive use could be from the female or the male, but the woman being the bearer of the burden of pregnancy and childbirth with the associated risk is less likely to be resistant to contraceptive use than the male counterpart. In Uganda, Kabagenyi, and co-workers reported that barriers to contraceptive use included: limited choices of available male contraceptives, fear, and concerns relating to vasectomy, perceptions that reproductive health was a woman’s domain due to gender norms and traditional family planning communication geared towards women, preference for large family sizes which are uninhibited by prolonged birth spacing; and concerns that women’s use of contraceptives will lead to extramarital sexual relations 10. The findings of Kabagenyi appear to mainly affect the male partner hence, the need to assess the opinion of men concerning contraceptive use by the couple.
Many pieces of research that attempted to examine the low use of contraception focused on the women, the roles of the government, and the healthcare givers, yet our contraceptive use rate in developing countries remained low. Though some, but not so many researchers, have looked in the direction of the male partner in proportions similar to that of female partners. Some of the research that investigated male partners showed that husbands could be barriers to contraceptive use by the couple. Therefore, it is necessary to assess husbands' knowledge about contraception, its acceptability to them, and their readiness to use it as a couple, hence the need for this study. An important question we want to answer is if the husband’s knowledge of contraceptives influences the use and attitude of the couple towards its use.
This Study aims to assess the knowledge of husbands on available contraceptive options, determine the proportion of husbands that have used contraceptives, and determine factors affecting the attitude of husbands towards contraceptive use by the couple.
METHODOLOGY
This was a cross-sectional study conducted in Ibadan North local government area of Oyo State. This local government accommodates the University of Ibadan, the University college hospital Ibadan, and the Bodija market, one of Nigeria's largest agricultural product markets. Therefore, the purposively selected sampling areas were locations around these three areas where many people in the city come to; for trading thus forming a fair representation of people in the city of Ibadan.
The study locations were the immediate environment of the University College Hospital (UCH) including the neighboring mechanic village, Mokola roundabout, and Sabo area of Mokola all of which are around UCH Ibadan; Bodija market, and the commercial area of Agbowo which is very proximal to the University of Ibadan. The sampling of the participants was restricted to work areas and open spaces. Entering houses was prohibited because of the possible hazards of entering unknown houses. The respondents were men who were married, divorced, or separated at the time of the interview. All consenting married men with their wives still in their reproductive ages at the time of the study were included as well as men who were once married but may have divorced or separated at the time of this survey. We excluded all non-consenting married men whose wives were in their reproductive ages.
A structured questionnaire that was both self and interviewer-administered was used for this study. The questionnaire was arranged in sections to obtain information about the socio-demographic characteristics of the respondents, their knowledge of contraceptive options, acceptance of contraceptive use, and factors affecting their use of contraceptives. Knowledge of contraception was categorized based on the knowledge of the uses of contraception which are to; prevent unwanted pregnancy, space childbirth, and prevent sexually transmitted infection. People who could state any two including preventing unwanted pregnancy are classed as having adequate knowledge; a person who knows only one function is grouped as having inadequate knowledge while a person who knows none is described as having “no knowledge”.
The questionnaire was pretested among the non-clinical staff of UCH Ibadan, who worked at the Human Resource Department; and no major change in the questionnaire was required. All the considerations of ethics were carefully ensured. Using the Leslie Kish formula and the prevalence of contraceptive use in men of 26% as reported by Shattuck et al 11, a sample size of 330 was calculated. An equal number of printed questionnaires were sent to the different research locations though with varying numbers of responses from the locations. The data collected was imputed into the data page of the statistical package for social sciences (SPSS) version 25.0. Descriptive statistics were performed using tables while categorical variables were analyzed using the Chi-Square test. The level of significance was judged at a p-value < 0.05.
RESULTS
Three hundred and forty- five men were interviewed; seven of them were single and thus, were excluded from the analysis. The remaining 338 men that were analyzed were married, separated, or divorced men.
Following the adjustment for age, the educational status of the husband and the wife, religion, and tribe; Yoruba men statistically
Table 1: Sociodemographic Characteristics of the respondents

significantly use contraception more than other men. (p: 0.006, 95%CI: 0.223 – 0.773).
Table 1 shows the sociodemographic characteristics of the three hundred and thirty-eight men interviewed. The mean age was 41.68 ± 11.01 years with about 70% between the ages of 30 to 49
Table 2: Knowledge of contraception among the respondents


years. Skilled and semi-skilled workers were 43.59% and 45.99% respectively. The majority of the respondents were Christians (56.51%), Yoruba by tribe (79.59%), and had tertiary education (62.92%) as well as their wives (59.94%). Nearly
Table 3: The use of contraception among the respondents
Table 3: The use of contraception among the respondents


all (99,40%) of the men were married at the time of the survey with the remaining 0.6% in equal proportion either divorced or separated. Most (90.80%) practiced monogamy and had at least a child (99.40%). About 21% earned at least one hundred and fifty thousand Naira monthly while about 15% earned less than twenty-five thousand naira monthly.
Table 4: Table of Associations between demographic variables and the knowledge and use of contraception among the respondents.

Table 2 shows the knowledge of contraception among the respondents. Most (91.10%) of the respondents have heard of contraceptives before, 87.30% reported that they know contraceptives and 78.02% had adequate knowledge of contraception.
Table 5: Binary logistic regression with knowledge of contraceptives as the dependent variable

After adjusting for age, the educational status of the husband and the wife, the religion, and the tribe; men with educated wives statistically have more knowledge of contraception than men whose wives are not educated (p: 0.04, 95%CI: 0.089 – 0.948).
Table 6: Binary logistic regression with attitude towards contraceptive use as the dependent variable

After adjusting for age, the educational status of the husband and the wife, the religion and tribe; men who are educated, Christians and of Yoruba tribe statistically significantly have better attitude towards contraception use than other men. (p: 0.004, 95%CI: 0.093 – 0.630), (p: <0.001, 95%CI: 0.175 – 0.530). (p: 0.016, 95%CI: 0.239 – 0.866)
Television and radio (51.20%) were the common sources of knowledge on contraceptives; other sources included education at health care facilities (32.20%), social media (31.90%), and discussion among peers (24.90%).
About four-fifths (84.64%) of the men were aware of male and female contraception. Male condoms (82.30%) followed by withdrawal method (82.30%) were the male methods mostly known to the men though about a quarter (25.70%) knew of male sterilization. Oral pills (64.76%) and
Table 7: Binary logistic regression with the use of contraception as the dependent variable
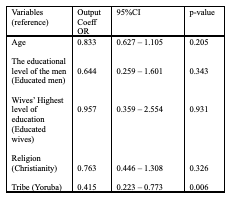
injectable (53.50%) were the female methods most known to the respondents, although about a quarter knew about tubal ligation. Almost three-fifth (56.20%) of the men used male condoms with their wives. Other contraceptives which the men knew their wives used were Emergency contraceptive pills (50.16%), injectables (47.47%), intrauterine devices (34.80%), tubal ligation (31.60%), and Jadelle (29.81%) among others. The majority of the men knew that contraception could prevent unwanted pregnancy (83.48%), be used for child spacing (83.04%), and is generally safe (58.68%) although 70.96% thought that contraceptives could fail while 74.77% thought that contraceptives are readily available.
About 65.68% of the men have used contraception before even though about 83% knew that contraception could prevent unwanted pregnancy and help in child spacing (Table 2). Of the 222 (65.68%) men (Table 3) who have previously used contraceptives, 161 (47.63%) have used them with their wives while about 61 (18.05%) had used them with other women apart from their wives. Almost three-fifth (57.10%) of the men have been using contraception for more than 10 years, while only about one-fifth (23.10%) have been using contraceptives for five years or less. About 31.37% of the men have not used any form of contraception in more than one year. As a couple, the commonly used contraceptive methods by the couple include male condoms (81.08%), withdrawal methods (72.07%), and contraceptives that are applied by the female partner (54.50%). Among the 161 men who knew the contraceptive methods adopted by their wives, the common methods used include oral contraceptive pills (36.65%), intrauterine devices (13.04%), injectables (18.63%), and emergency pills (22.36%).
Most of the men (84.35%) knew that contraceptives are not free, but are however affordable (Table 2). Among the 68.66% that agreed with the couple’s use of contraceptives, the common reasons are to prevent unwanted pregnancy and child spacing (70.87%). Of the 105 men (31.07%) who would not agree with contraceptive use themselves, the common reasons given included cultural, religious, moral, and social beliefs respectively (20%), (33.33%), (13.33%), and (9.52%). Almost a fifth (18.10%) believed that contraceptives make sexual pleasure to be incomplete. The reasons why men do not want their wives to use contraceptives is similar to the reason why men themselves do not want to use contraceptives; others include fear of possible impairment of future fertility (66.67%). Most of the men (88.50%) expect that their wives must seek their consent before taking any form of contraception, though 72.20% of the men think it is also necessary to inform their wives before using contraceptives.
More than 90% of men from each of the tribes interviewed knew about contraception and there is no significant difference in their knowledge (p = 0.963). About 92.20% of the men with four or more children knew about contraception while about 90.90% of men with less than four children knew about contraception, but this difference is not statistically significant (p = 0.70). About 91% of women with at least secondary education knew about contraception compared with 81.40% among those men whose highest level of education is a primary school and this is statistically significant (p = 0.04). Furthermore, 91.30% of the men whose wives had at least secondary school education known about contraception compared with 81% among the men whose wives did not have more than primary school education and this is statistically significant (p = 0.043). The use of contraception increased progressively with the age of the men with the highest use being among men aged 40 – 49 years (71.10%), thereafter there is also a progressive decline in contraceptive use. There is a statistically significant association between age and contraceptive use (p = 0.004). Over 70% of men with less than four children used contraception compared with 59% among men with four or more children, and this difference is statistically significant (p = 0.021). Religion does not influence contraception use among the respondents (p = 0.16). Almost 70% of men whose wives had at least secondary education used contraception compared with 46.20% among men whose wives did not have more than primary school education; this is statistically significant (p = 0.005). More (72.40%) of the men earning more than one hundred-thousand-naira monthly use contraception compared with 67.10% among men that earn less than that amount however this is not statistically significant (p = 0.3335). The Yorubas and Igbos used contraception more significantly than any other tribes captured by the study (p < 0.0001). Approximately 70% of the men who had at least secondary education used contraception compared with 46.30% among the men whose highest level of education was primary school.
DISCUSSION
The mean age of the respondents was 41.68 ± 11.01 years, though higher than the men’s mean age of 39.8 years that was reported in Ethiopia 12, nonetheless; they are within the same age range, and thus comparable. These interviewed men were also of the same age range as reported in Nigeria 13,14 and Uganda 10,15 though some did not report mean age but reported median age.
About 91.10% of our respondents have heard of contraception before though 87.30% knew contraception in form of having seen one before beyond just hearing about it, and about 78.02% knew that contraception could help to prevent unwanted pregnancy, space childbirth, and prevent sexually transmitted infection, which constituted good knowledge. The level of knowledge could be assessed as being good. This good knowledge could be attributable to high educational status since over three-fifth of the respondents had tertiary education, with only very few having no education. In addition, apart from the men being educated most of their wives also had tertiary education and this is another positive factor that probably enhanced the good level of knowledge. This level of knowledge is higher than 58 % reported among men in Kenya, 43 % in Nigeria, and 27 % in Senegal 16. This could be because our study was conducted in the urban part of the country thus excluding the rural dwellers. The design of individual studies could also have affected the reported prevalence of knowledge because the studies in Uganda were Focused-Group Discussion (FGD), and In-depth Interviews which are more involving than the cross-sectional study design of this research.
Television, radio, and social media constituted the source of information on contraception for about 83% of the respondents and this might likely have contributed to the high level of knowledge since most people have access to these means of information dissemination. This is in sharp contrast to the finding of Thummalachetty et al in Uganda where the commonest source of contraceptive knowledge for the men was from their partners especially when they complained of side effects, their peers, or hearsay 15. Perhaps not just educational level but more importantly cultural beliefs could have contributed to this belief that contraception matters are women’s business. The Minority in this Uganda study obtained their information from health providers and mass media campaigns 15.
The majority (82.30%) of the men knew male condoms and this could be because it is perhaps the cheapest, most accessible form of contraception, and use is very easy. The experience is similar in Uganda 15. Oral pills (64.76%) are the female contraceptive method most known to the interviewed men. This could also be because it is cheap, readily available in the street, and does not interfere with the act of intercourse. Next to pills, 53.50% of the men knew injectables; this could also possibly be because it also does not interfere with the act of intercourse, and with the availability of Sayana press, a self-administered injectable containing Depo Medroxy progesterone Acetate, it is very easy for the women to collect or buy the steroid from the healthcare facility as the case may be and then inject themselves at home without the help of any healthcare giver; and this confers protection for at least 3 months. This additional flexibility with injectables may have contributed to its increased awareness among the interviewed men. In Uganda, Depo Medroxyprogesterone acetate injection is the most popularly used 15. The poor knowledge of vasectomy among the interviewed men though a procedure for males may be a reflection of the aversion of men to surgery, or the idea that it is a permanent form of male contraception, though it could also be a reflection of the level of awareness created by the healthcare workforce because one thing is to know about it and another thing is to be willing to accept the method. Kabagenyi et al also reported aversion in Uganda, not for only vasectomy, but even for male condoms 10.
Of the 338 men interviewed, 222 (65.68%) have used contraception before, though 161(47.63%) have used it with their wives, representing about 72.50% of those men who had used contraception before. Of these 161 men, 101 men (62.73%) used it occasionally, while only 60 men (37.27%) used contraception every time. The 116 men (34.32%) that have not used any contraception at all, and the 101 men (29.88% of the total studied population) that used contraception occasionally may be men who earnestly desired their wives to get pregnant at the time of this study, and this may explain the non-use and inconsistent use as the case may be for the men. This can be understood better knowing that the mean age of the interviewed men was 41 years, so non-contraceptive use may be in pursuit of fertility because; whereas it is a little easy to know the average age at which men become fathers, it is extremely difficult to determine the average age at which men have their last child because of many factors 17. More than half (57.10%) of the 161 men that have used contraception before have been using it for more than 10 years while more than 70 centiles have been using it for more than 5 years. These may reflect men who early enough have been using contraception to space their children, and or those who have been using it to prevent infection with sexually transmitted infections or do not have the desire to impregnate a woman despite having their sexual desire met. The long use of contraception may also be a reflection of the fact that some of the methods, especially the pills and barrier methods, are readily accessible to men. Fifty-nine percent of the men interviewed in Uganda had used contraception, which is slightly lower than 65.68% in this study. However, a small sample size of 46 participants could have negatively affected the result obtained in Uganda by Thummalachetty and co-workers 15.
Check spacing of the new paragraph
Men with at least secondary school education and those whose wives add at least secondary education are more aware of contraception than those whom neither they nor their wives were that schooled. Contraceptive use by men was also significantly influenced by the educational status of their wives with better use noted among men whose wives had more than primary education. This further confirms the saying that knowledge is wealth, and that ignorance is a disease. The more educated the wives are the more likely the man would use contraception. This could be because educated women may have better skills and wisdom to persuade their husbands to see the benefits of contraception and in so doing encourage them to use it more. Though the knowledge of contraception is not affected by tribe among the respondents, however, contraception use was significantly higher among Yoruba and Ibo men than among Hausa men. This might be related to the desired family size of each man. Because men in northern Nigeria have larger family sizes than any other part of the country 18,19, the low contraceptive use among the Hausa men in this study did not correlate with the good knowledge they had and may just be their attempt to complete their desired family size before up-taking any form of contraception.
Men with less than 4 children used contraception more than those with more than four children. This could be a real demonstration of the desire to control the family size such that those who do not want to have more than 3 children or who desire to space their children are more committed to the use of contraception, whereas; men with children of more than 4 who still use contraception less frequently may be men who are not motivated about family planning or men who desire a large family size; however, Thummalachetty reported a contrary finding with contraceptive use higher among men with large family size 15. Though monthly income did not influence contraception use maybe because some government facilities give them for free or at a highly subsidized rate; however, the more educated men used contraception than the non-educated ones. This further buttresses the fact that education is a key part of advocacy. Beyond the jingles on radio and television, a more educated person will likely be able to read more about contraception on social media and even medical journals and in so doing receive more understanding of the benefits of contraception.
Of the 222 (65.68%) men who have previously used contraceptives, 161 (47.63%) have used them with their wives while about 61 had used them with other women apart from their wives and this may further reinforce the belief of the respondents that contraceptive can prevent unwanted pregnancy.
The educational level of the wives influences the knowledge of contraception by the man with the husbands of the educated women having better knowledge, while good attitude towards contraceptive use is enhanced by the educational level of the men as well as their tribe and religion with being educated, being a Christian
and also of Yoruba tribe as being of positive effects. The use of contraception is affected by the tribe, with use being higher among the Yoruba respondents, though this could be because the study was conducted in the southwest of Nigeria where Yoruba is the dominant tribe.
CONCLUSION
The majority of the interviewed men were aware of contraception, however, this knowledge did not translate significantly to contraception use among the men, because a smaller number of the aware men utilized contraception.
The main limitations to contraception used were the age of the man, cultural barriers, family size, and the educational status of both husband and wife. The higher the wives’ education, the more knowledge of contraception the men heard. Higher education of the couple as well as being a Christian and a Yoruba increases a good attitude towards contraception use. However, being a Yoruba is a positive influence on actual contraception use.
REFERENCES
- Jain R and Muralidhar S. Contraceptive Methods: Needs, Options and Utilization. The Journal of Obstetrics and Gynecology of India. 2011: 61(6):626–634.
- Obilor N. M., and Osita-Njoku A. Contraceptive Use in Low- and Middle-Income Countries: The Roles of Socio-Economic Inequalities, Cultural and Religious Belief. GSJ. 2021;9(10):1194–209.
- Kriel Y, Milford C, Cordero J, Suleman F, Beksinska M, Steyn P, et al. Male partner influence on family planning and contraceptive use: perspectives from community members and healthcare providers in KwaZulu-Natal, South Africa. Reprod Health. 2019; 16(89). Available from: https://doi.org/10.1186/s12978-019-0749-y
- Annual report 2014 | United Nations Population Fund [Internet]. [cited 2022 Jul 27]. Available from: https://www.unfpa.org/annual-report-2014
- Family planning/contraception methods [Internet]. [cited 2022 Jul 27]. Available from: https://www.who.int/news-room/fact-sheets/detail/family-planning-contraception
- Kantorová V, Wheldon MC, Ueffing P, Dasgupta ANZ. Estimating progress towards meeting women’s contraceptive needs in 185 countries: A Bayesian hierarchical modeling study. PLoS Medicine. 2020 Feb 18;17(2).
- World Health Organization (WHO) Contraception [Internet]. [cited 2022 Jul 27]. Available from: https://www.who.int/health-topics/contraception#tab=tab_1
- Nations Department of Economic U, Affairs S, Division P. World Fertility and Family Planning 2020: Highlights.
- Aliyu AA, Dahiru T, Oyefabi AM, Ladan AM. Knowledge, determinants and use of modern contraceptives among married women in Sabon Gari Zaria-Northern Nigeria. Journal of Medicine and Biomedical Research. 2015;14(2):13–21.
- Kabagenyi A, Jennings L, Reid A, Nalwadda G, Ntozi J, Atuyambe L. Barriers to male involvement in contraceptive uptake and reproductive health services: a qualitative study of men and women’s perceptions in two rural districts in Uganda. Reproductive Health 2014 11:1 [Internet]. 2014 Mar 5 [cited 2021 Nov 10];11(1):1–9. Available from: https://reproductive-health-journal.biomedcentral.com/articles/10.1186/1742-4755-11-21
- Shattuck D, Kerner B, Gilles K, Hartmann M, Ng’ombe T, Guest G. Encouraging contraceptive uptake by motivating men to communicate about family planning: The Malawi Male Motivator project. American Journal of Public Health. 2011 Jun 1;101(6):1089–95.
- Tuloro T, Deressa W, Ali A, Davey G. The role of men in contraceptive use and fertility preference in Hossana Town, southern Ethiopia. 2009;(October).
- Akpamu U, Nwaopara AO, Otamere HO, Osifo UC, Adisa AW, Okhiai O AE. Awareness of Contraceptive Methods amongst Married Male Population of Ekpoma, Nigeria. Afr J Biomed Res. 2011;14(May):131–5.
- Ezeanolue EE, Iwelunmor J, Asaolu I, Obiefune MC, Ezeanolue CO, Osuji A, et al. Impact of male partner’s awareness and support for contraceptives on female intent to use contraceptives in southeast Nigeria. BMC Public Health [Internet]. 2015;1–6. Available from: http://dx.doi.org/10.1186/s12889-015-2216-1
- Thummalachetty N, Mathur S, Mullinax M, Decosta K, Nakyanjo N, Lutalo T, et al. Contraceptive knowledge, perceptions, and concerns among men in Uganda. BMC Public Health [Internet]. 2017 Oct 10 [cited 2022 Jul 18];17(1). Available from: /pmc/articles/PMC5633881/
- Okigbo CC, Speizer IS, Corroon M, Gueye A. Exposure to family planning messages and modern contraceptive use among men in urban Kenya, Nigeria, and Senegal: a cross-sectional study. Reproductive Health [Internet]. 2015;1–11. Available from: http://dx.doi.org/10.1186/s12978-015-0056-1
- Schweizer V. 30 Years of Change in Men’s Entry into Fatherhood, 1987-2017. 2019 Dec [cited 2022 Jul 15]; Available from: https://www.bgsu.edu/ncfmr/resources/data/family-profiles/schweizer-years-change-mens-entry-fatherhood-fp-19-28.html
- Household Population and Housing Characteristics | 11.
- NLSS. Nigeria Living Standards Survey A Survey Report by the Nigerian National Bureau of Statistics (in collaboration with the World Bank). Natl Bur Stat [Internet]. 2020;12(2):1–18. Available from: http://dx.doi.org/10.1016/j.rser.2015.07.050%0Ahttp://documents.worldbank.org/curated/en/2013/05/ 17765643/global-tracking-framework-vol-3-3-main-report%0Awww.humangeo.su.se%0Ahttp://infinitypress.info/index.php/jas/article/viewFile/1316/593%0Ahttps://ep

